Advances in Spinal Surgery

Dr Paul Thng Leong Keng 
MBBS (Singapore)
FRCS (Edin)
FRCS (Glas)

Minimally Invasive Spine Surgery (MISS)
Equipment and technology used in surgery has improved tremendously over the last few decades. This has allowed certain traditional surgeries to be done through small or minimal incisions.

The avoidance of longer incisions results in less tissue/muscle damage during the surgery. This often results in several potential benefits:
- Faster healing/recovery and less post-operative pain.
- Less blood loss from surgery
- Better cosmetic results
- Less consumption of pain medication after surgery
Some examples of surgeries that can be performed through a minimally invasive approach:
- Decompression surgery (e.g. in spinal stenosis or herniated/”slipped” disc)
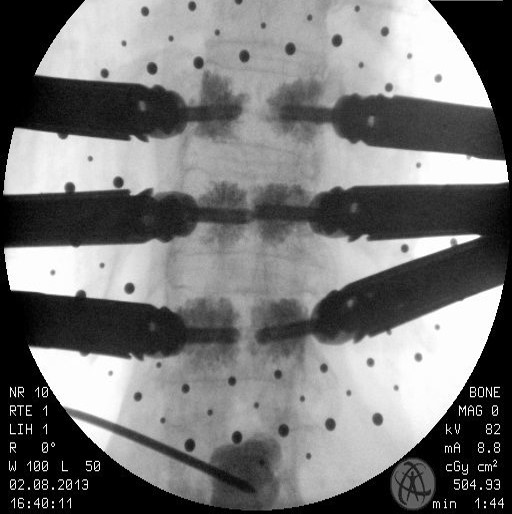
- Insertion of pedicle screws (e.g. spinal fractures or spinal tumour management)
- Spinal fusion surgery (e.g. Transforaminal Lumbar interbody Fusion or TLIF)
- Spinal injections (diagnostic or therapeutic)
- Vertebroplasty and kyphoplasty for vertebral compression fractures
Limitations
As technology improves more and more spine surgery can be performed in the minimally invasive manner. But certain more complex surgeries may still require the more traditional incision and “open” surgery. Minimally invasive surgery may also sometimes require more time for the procedure.
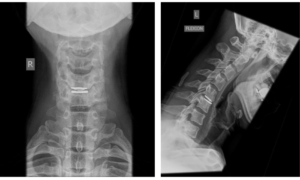
Artificial Disc Replacement
When an intervertebral disc degenerates, it sometimes can cause symptoms. Most of these can be managed non-operatively. However, a significant proportion of these might require surgery, especially if non-operative measures fail to bring about relief. One of the options of surgery is to do a spinal fusion. This eliminates movement in the spinal segment. Often, a spinal decompression may accompany a spinal fusion.
The disadvantage of a spinal fusion is that it makes the segment rigid. An artificial disc replacement allows surgery to be performed, and instead of fusion, a disc-like device is inserted that allows the body to maintain motion at that segment. This has the theoretical advantage of maintaining movement. The results of studies are still on-going as this is still a relatively new technology. For example, in the cervical spine, the ongoing US IDE trials suggest that the interim term results (4-5 years) of the cervical disc replacement is superior to fusion, but more long term results are still required.
Limitations
The disc replacement surgery is a spine surgery that carries with it all the potential complications of spine surgery, including (but not an exhaustive list) infection, bleeding, nerve injury, soft tissue injury and implant –related issues. It also should not be used in conditions of infection, tumour or spinal instability. Please discuss with your doctor with regards to suitability of a disc replacement for your condition.
Spinal Navigation Imaging
Spinal instrumentation (most commonly the insertion of pedicle screw constructs) have made great advances in the last 2 decades, and is common as part of spinal surgery today. Convention methods usually relied on X-rays/fluoroscopy or on the surgeon’s skill and experience to properly place the spinal instrumentation. Spinal navigation is a tool which allows the surgeon real-time visualization of the spine during surgery during the insertion of spinal instrumentation. This increases the accuracy and safety of spinal instrumentation during surgery. It also potentially allows the use of less radiation for the surgery
Spinal navigation can be performed either in a 2-D or 3-D imaging fashion.
Limitations
Most spinal navigation systems require a series of steps before usage, involving preparation, registration, ensuring sterility. All these steps take extra time. The extra usage of equipment also will incur increased costs. Also, for the surgeries that do not require spinal instrumentation spinal navigation is then of limited use.
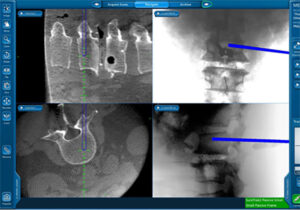
eg. 3D spinal navigation during insertion of pedicle screws during spine surgery
Spinal Neuromonitoring / Spinal Cord Monitoring
Spinal neuromonitoring is a procedure that can be used during spinal surgery. Its main purpose is to detect possible injuries to the spinal cord or nerves during the surgery. This is done by placing electrodes on the patient’s skin and muscles. The electrodes are then connected to a computer which can detect changes in the patient’s nervous system. The computer can also send a stimulus to the patient and by watching the response possible damage to the nerves might be detected. The monitoring of the computer is usually performed by a doctor trained in the procedure who can then give feedback to the operating team and necessary corrective measures taken.
There are 3 commonly used neuromonitoring modes
- SSEP (somatosensory evoked potentials)
- TcMEP (Transcranial motor evoked potentials)
- EMG (electromyography)
Limitations
Each of these modes monitor different nerves and pathways in the spinal cord and can be affected under different circumstances. For example, the SSEPs usually monitor the neural pathways from the limbs to the brain usually through the dorsal column (a section of the spinal column). While it is reliable and generally not affected by anaesthesia, it may not reliable in monitoring some of the motor pathways at the front (anterior) of the spinal cord. The TcMEP is better at monitoring the motor pathways but may be affected by general anaesthesia
The interaction between the neuromonitoring team and the operating team also takes time, which may lead to a prolongation of the operation.
While the neural pathways for SSEP and TcMEP are well established, at present there is limited published data to show that patient outcomes are improved. It is therefore likely to be more useful when the risk of injury to the spinal cord is high, but less useful when the risks are lower.
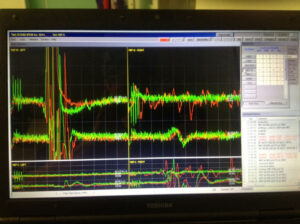
E.g. of TcMEP during spinal surgery

Dr Paul Thng Leong Keng
Dr. Thng has been recognized for his work internationally and has been invited to demonstrate live spine surgical and operative skills in several countries
- Senior Consultant and Medical Director, PTL Spine & Orthopaedics Clinic
- Visiting Senior Consultant Orthopaedic Surgeon, Changi General Hospital
- Adjunct Associate Professor, National University Hospital
- Trustee, AO Foundation
- Associate Editor, Global Spine Journal
- Scientific Reviewer, Singapore Medical Journal and Annuals of the Academy
Dr Paul Thng Leong Keng is a fellowship-trained orthopaedic surgeon subspecializing in spinal surgery. Based on hospital OTM records from 2003-2013, he performed over 3000 operations and over 1200 spine procedures, both open and minimally invasive. He has held various prestigious positions such as the Head of Spine service at Changi General Hospital, Chairman of AOSpine East Asia, and Executive Member of AOSpine International Board.
Dr. Thng has been recognized for his work internationally and has been invited to demonstrate live spine surgical and operative skills in several countries. He continues to contribute to the field through research and serves as an associate editor of the Global Spine Journal.
PTL Spine & Orthopaedics
Mount Elizabeth Novena Specialist Centre
38 Irrawaddy Road #07-34
Singapore 329563
Make An Appointment
For enquiries or feedback, please fill the following form below and we will get back to you as soon as we can.